
دانلود رایگان مقاله ارتباط بین نتایج درک شده بیمار و تغییرات بیومکانیکی
چکیده:
سابقه: عمل جراحی جایگزینی کل زانو(TKR) در جوانان، یعنی جمعیتی فعال تر با انتظارات کاربردی بیشتر استفاده شد. فهم اینکه آیا ارزیابی درک-بیمار از وظایف، منعکس کننده اهداف ارزیابی بیومکانیکی می باشد که در فهم مهم است یا محدودیت های عملکرد می تواند به اندازه کافی در محیط بالینی کنترل شود.
سوالات تحقیق: آیا تغییرات در ارزیابی اهداف بیومکانیکی گام ارزیابی نتایج بیمار-گزارش شده در حدود 12 ماه بعد از عمل جراحی TKR را منعکس می کند ؟
شیوه ها: تجزیه و تحلیل گام سه بعدی با OA بر روی 41 بیمار انجام شد، که برای عمل جراحی TKR برنامه ریزی شده بود، 22 نفر از آنها برای ارزیابی های بعدی (9 تا 24 ماه) برگشت خورده بودند. تجزیه و تحلیل اصلی اجزاء برای تعریف ویژگی های تناوب بین افراد مبتلا به OA به علاوه کنترل 31 فرد غیر-آسیب شناختی برای آموزش طبقه بندی کاردیف، تکنیک دسته بندی عینی، استفاده شد و سپس تغییرات بعد از عمل جراحی را حساب می کند یا می شمارد. تغییرات-درک بیمار همچنین با استفاده از شکاف زانو در آکسفورد (OKS)، بررسی نتایج زانو(KOS)، و امتیازات سیستم جمع آوری رسیدگی درد(PACS).. ضرایب همبستگی پیرسون و اسپیرمن برای ایجاد روابط بین تغییرات در نتایج درک شده و بطورعینی-ارزیابی شده محاسبه شد.
نتایج: ارزیابی عینی تغییرات بیومکانیکی به شدت مرتبط با تغییرات در OKS(r=-0.695، p < 0.001) و نتایج ارزیابی شده KOS (r=-.810، p < 0.001) می باشد. درد(PACS) تنها مرتبط با وظایف بیومکانیکی بعد از عمل جراحی می باشد (r=-.623, p=0.003).
اهمیت: در این مطالعه بیومکانیک، رابطه بین تغییرات در عملکرد یا وظایف عینی و ارزیابی گزارش شده بیمار قبل و بعد از عمل جراحی TKR قوی تر از مطالعاتی است که شامل متریک بیومکانیک نمی باشد. کیفیت حرکت ممکن است اهمیت بیشتری برای بهبود درک بیمار از ارزیابی عملکرد داشته باشد که تنها زمان گرفته شده یا فاصله حرکت در مدت فعالیت های اصلی را بررسی می کند.
1.مقدمه
اهداف اصلی تعویض کامل زانو (TKR) در درمان ورم مفاصل و استخوان ها زانو (OA) بهبود کیفیت زندگی از طریق ترمیم عملکرد مفصل و کاهش درد می باشد. در سالهای اخیر، افزایش چشمگیری در کاربرد TKRبرای درمان افراد جوانتر[1], و افرادی با انتظارات اصلی بالاتر[2,3] وجود دارد. تغییرات در عملکرد فیزیکی بعد از جراحی بطورمعمولی با استفاده از ارزیابی نتایج گزارش شده بیمار نظارت میشود(PROMs) . مدارک اخیر عیوب PROMs برای کنترل تغییرات در عملکرد مبتنی بر ارزیابی های بعد از عمل جراحی TKR[4–7] نشان می دهد. آن همچنین پیشنهاد می کند که بیماران با OA شدید سختی در تمایز بین محدودیت اصلی و درد دارند زمانیکه توانایی خود را برای انجام فعالیتهای زندگی روزمره خود-ارزیابی می کنند[4].
تجزیه و تحلیل گام رویکرد عینی برای ارزیابی اختلاف آشکاربین عملکرد مبتنی و تغییرات اصلی درک شده قبل و بعد از عمل جراحی TKR ارائه می دهد. مطالعات زیادی عیوب اصلی در پارامترهای بیومکانیکی در گروهای TKR در زمان مقایسه با افراد سالم گزارش کرده اند[8]. به هرحال، چند مطالعه بحث کرده است که آیا بیماران با بهترین بهبود درک شده همچنین بهترین نتایج بیومکانیکی و برعکس را دارند.
تجزیه و تحلیل بیومکانیگی گام اطلاعاتی در مورد سینیتیک و حرکت شناسی مفصل تولید می کند، اما تفسیر یافته ها با وابستگی متغیرهای بیومکانیکی مشکل می شود[9]. در نتیجه، منافع زیادی در تکنیک های آماری وجود دارد که به طور عینی تغییرات گام های آسیب شناسی را مربوط به جمعیت هنجار خلاصه می کند[9–11]. یکی از چالشها برای خلاصه کردن داده بیومکانیکی کاهش موجی شکل موقت به متریک مجزا است. یک شیوه مشهور تجزیه و تحلیل اجزای اصلی(PCA) است، که داده ها را به اجزای متناوب قائم کاهش می دهند. این شیوه عینی است، بنابراین نیازی به انتخاب معقول ویژگی های هدف ندارد مانند حداکثر طول موج، و در مطالعات زیادی نشان داده شده است که بطور موفقیت آمیزی تفاوت ظریف بین الگوهای جنبشی را شناسایی می کند[12,13].
در واحد ما، کاربرد PCA با شیوه طبقه بندی شده مبتنی بر نظریه دمپستر-شافر مدارک ترکیب شده است، که "دسته کننده کاردیف" نامیده می شود. این شیوه نشان داده شده است که به درستی تغییرات بیومکانیکی در مرحله-اخیر افراد مبتلا به OA[14] به عنوان پایه ای برای بهبود ارزیابی بعد از TKR [15–17]مشخص می کند. اجرای تکنیک های مذکور برای بیومکانیک های اعضای پایین در مدت سطح گام، اختلاف بین اهمیت بهبود اصلی عینی و ذهنی تاکید می کند[16]. به هرحال، اهداف واقعی گرا بعد از عمل جراحی ممکن است ارزیابی نتایج ذهنی و عینی تفاوت داشته باشد. بر فرض مثال، (OKS) بویژه برای تغییرات درک شده بعد از عمل جرا حی شکاف زانو آکسفورد در TKR واکنشی طراحی شده است ، بدین معنی که افراد سالم به باند باریک با ارزیابی نتایج افت می کنند، بطورکلی امتیاز کامل0/48 حاصل می شود. شیوه های عینی مانند دامنه حرکت زانو یا طبقه بندی گام، به هرحال، بطور ویژه طراحی نشده اند تا در تغییرات بعدی TKR واکنشی باشند، بنابراین افراد سالم بطورکلی در سهم بزرگی از ارزیابی نتایج کاهش می یابند.
این مطالعه قصد دارد تا نتایج حاصل از بیمار و دسته بندی بیومکانیکی عینی از سطح گام را ارزیابی کند. اولین هدف مقایسه سطح تغییرات در PROMs و دسته بندی بیومکانیکی سطح گام بعد از عمل جراحی TKR می باشد. هدف دوم بررسی اینکه آیا ارزیابی منافع اصلی بعد از جراحی بطورقابل توجهی با استفاده از دسته بندی گام در مقایسه با تنها استفاده PROM تغیر یافته است یا خیر.
2. شیوه ها
2.1 شرکت کنندگان در مطالعه
مطالعه با استفاده از کمیته اصول اخلاقی تحقیق از گروه سلامت دانشگاه های وال، کاردیف و ولز تایید شد. 41 بیمار با بیماری زانو OA که برای عمل جراحی اولیه TKR در مرکز ارتوپدیک (استخوان پزشکی) وال و کاردیف فهرست شده، برای مطالعه به کار گرفته شدند. آنها برای افرادی که قادر به قدم زدن 10 متر بدون عصا بودند، استثناء قائل شدند، قادر به اطلاع رسانی بطوررضایتبخشی نبودند، آنها دارای ارتريت روماتيسمي، یا اسکلتی عضلانی غیر مرتبط، شرایط بصری یا عصبی دارند که ممکن است بر شیوه های حرکت آنها تاثیر بگذارد. شرکت کنندگان با OA دو جانبه مستثنی نبودند، نه مواردی که آرتروپلاستی را در سایر اعضای مشترک پایین تحمل کرده اند. در زمان تجزیه و تحلیل، 22 نفر ارزیابی مجدد حداقل 9 ماه بعد از عمل جراحی را تحمل کرده اند. به علت مسائل عملی زیادی، تغیرپذیری در زمان ویزیت بیمار پس از تشخیص یا درمان—میانگین زمانی 13.2 ماه بود به هرحال این دامنه بین 9.3 و 22.8 ماه بعد از عمل جراحی بود.
سی و یک داوطلب بدون آسیب شناسی اعضای پایین (NP) از کارمندان دانشگاه، دانشجویان و جامعه گسترده تر با استفاده از چسترها و ایمیل های تبلیغاتی تجهیز شدند. افراد مستثنی بودند اگر آنها سوابقی از شرایط اسکلتی عضلانی اعضای پایین داشتند که نیازمند درمان پزشکی، درد خود-گزارشی در اعضای پایین یا پشت یا شرایط بصری یا عصبی، اشتعالی دارند که ممکن است بر شیوه ای که آنها حرکت می کنند تاثیر بگذارند.
2.2 تجزیه و تحلیل بیو مکانیکی
تجزیه و تحلیل حرکت بشر در مدت سطح گام در تجزیه و تحلیل آزمایشگاهی حرکت در دانشکده کاردیف مهندسی انجام شد. مجموعه علائم اعضای پایین CAST[18] برای افراد پیوست شد، در حالیکه آنها پابرهنه در گام خود-ارزیابی در امتداد مسیر 10 متر قدم می زدند. مسیر های مارکر با استفاده از8 دوربین Oqus (Qualisys, Sweden) با سرعت 60 Hz جمع آوری شد و نیروی واکنش زمینی از دو نیرو سکو (برتک، آمریکا) با سرعت 1080 Hz محاسبه شد. مفصل ران، زانو سینماتیک وسینتیک قوزک پا با 3D بصری محاسبه شد. (حرکت C، آمریکا)
ABSTRACT
Background: Total Knee Replacement (TKR) surgery is being utilised in a younger, more active population with greater functional expectations. Understanding whether patient-perceived measures of function reflect objective biomechanical measures is critical in understanding whether functional limitations can be adequately captured within a clinical setting.
Research Question: Do changes in objective gait biomechanics measures reflect patient-reported outcome measures at approximately 12 months following TKR surgery?
Methods: Three-dimensional gait analysis was performed on 41 patients with OA who were scheduled for TKR surgery, 22 of which have returned for a (9–24 month) follow-up assessment. Principal Component Analysis was used to define features of variation between OA subjects and an additional 31 non-pathological control subjects. These were used to train the Cardiff Classifier, an objective classification technique, and subsequently quantify changes following TKR surgery. Patient-perceived changes were also assessed using the Oxford Knee Score (OKS), Knee Outcome Survey (KOS), and Pain Audit Collection System scores (PACS). Pearson and Spearman correlation coefficients were calculated to establish the relationship between changes in objectively-measured and perceived outcome.
Results: Objective measures of biomechanical change were strongly correlated to changes in OKS(r=-0.695, p < 0.001) and KOS(r=-.810, p < 0.001) assessed outcomes. Pain (PACS) was only related to biomechanical function post-operatively (r=-.623, p = 0.003).
Significance: In this biomechanics study, the relationship between changes in objective function and patientreported measures pre to post TKR surgery is stronger than in studies which did not include biomechanics metrics. Quality of movement may hold more significance for a patient’s perception of improvement than functional measures which consider only the time taken or distance travelled during functional activities.
1. Introduction
The principal goal of Total Knee Replacement (TKR) in the treatment of knee osteoarthritis (OA) is to improve quality of life through the restoration of joint function, and reduction of pain. In recent years, there has been a dramatic rise in the utilisation of TKR to treat younger patients [1], and those with higher functional expectations [2,3]. Changes in physical function following surgery have most commonly been monitored using patient-reported outcome measures (PROMs). Recent evidence suggests PROMs fail to capture changes in performance-based measures following TKR surgery [4–7]. It has also been suggested that patients with severe OA have difficulty discriminating between functional limitation and pain when self-assessing their ability to perform activities of daily living [4].
Gait analysis provides an objective approach for assessing the apparent disparity between performance-based and perceived functional changes pre to post TKR surgery. Numerous studies have reported functional deficits in biomechanical parameters in TKR cohorts when compared to healthy subjects [8]. Few studies, however, have discussed whether patients with the greatest perceived recovery also have the best biomechanical outcomes and vice versa.
Biomechanical gait analysis yields a wealth of information regarding joint kinematics and kinetics, but the interpretation of findings is complicated by interdependencies of the biomechanical variables [9].
As a consequence there has been growing interest in statistical techniques which objectively summarise pathological gait changes relative to normative population [9–11]. One of the challenges to summarising biomechanical data is the reduction of temporal waveforms into discrete metrics. One popular method is Principal Component Analysis (PCA), which reduces data into orthogonal components of variation. This method is objective, therefore requiring no subjective selection of target features such as waveforms peaks, and has been demonstrated in numerous studies to successfully identify subtle differences between movement patterns [12,13].
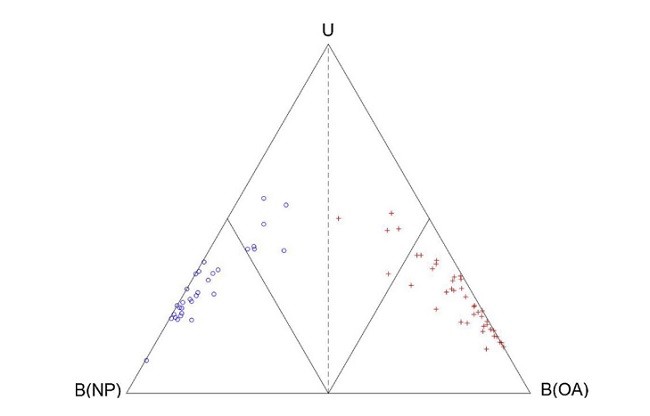
In our unit, the application of PCA has been combined with a classification method based on a Dempster-Shafer theory of evidence, termed the ‘Cardiff Classifier’. This method has been demonstrated to accurately characterise the biomechanical changes in late-stage OA subjects [14] as a basis for measuring recovery following subsequent TKR [15–17]. Applying these techniques to lower-limb biomechanics during level gait, disparities between the magnitude of subjective and objective functional recovery have been highlighted [16]. Realistic goals following surgery may, however, differ between objective and subjective outcome measures. For example, the Oxford Knee Score (OKS) is designed specifically to be responsive to perceived changes following TKR surgery, meaning healthy subjects would fall into a narrow band within the outcome measure, generally achieving a perfect score of 0/48. Objective methods such as knee range of motion or gait classification, however, are not designed specifically to be responsive to changes following TKR, hence healthy subjects generally fall within a larger portion of the outcome measure.
This study aims to assess the relationship between patient-perceived outcome and objective biomechanical classification of level gait. The first objective is to compare the level of change in PROMs and of biomechanical classification of level gait following TKR surgery. The second objective is to address whether the assessment of functional gains following surgery is significantly altered using gait classification in comparison to using PROMs alone.
2. Methods
2.1. Study participants
The study was approved by the Research Ethics Committee for Wales and Cardiff and Vale University Health Board. Forty-one patients with knee OA who were listed for primary TKR surgery at Cardiff and Vale Orthopaedic Centre were recruited into the study. Subjects were excluded if they were unable to walk 10 m without a walking aid, were unable to give informed consent, had rheumatoid arthritis, or had an unrelated musculoskeletal, neurological or visual condition which might affect the way they move. Participants with bilateral OA were not excluded, nor were those whom had undergone previous arthroplasty in other lower limb joints. At the time of analysis, 22 subjects had undergone re-assessment at least 9 months post-operatively. Due to several practical issues, there was variability in the timing of follow-up visit – the median time was 13.2 months however this ranged between 9.3 and 22.8 months following surgery.
Thirty-one volunteers with no lower-limb pathology (NP) were also recruited from University staff, students and the wider community using poster and email advertisements. Subjects were excluded if they had a history of a lower-limb musculoskeletal condition which required medical treatment, had self-reported pain in the lower-limb or back, or had an inflammatory, neurological or visual condition which might affect the way they move.
2.2. Biomechanical analysis
Human motion analysis was performed during level gait at the motion analysis laboratory at Cardiff School of Engineering. A lowerlimb CAST marker set [18] was attached to subjects, while they walked barefoot at a self-selected pace along a 10 m walkway. Marker trajectories were collected using 8 Oqus (Qualisys, Sweden) cameras capturing at 60 Hz, and ground reaction forces were calculated from two force platforms (Bertec, USA) capturing at 1080 Hz. Hip, knee and ankle kinematics and kinetics were calculated within Visual 3D (CMotion, USA).
چکیده:
1.مقدمه
2. شیوه ها
2.1 شرکت کنندگان در مطالعه
2.2 تجزیه و تحلیل بیو مکانیکی
2.3 نتایج بیمار گزارش شده
2.4 کاهش داده
2.5 دسته بندی داده
2.6 تجزیه و تحلیل آماری
3. نتایج
4.بحث
4.1 بیومکانیک گام و وضعیت اصلی درک شده
4.2 درد حس شده و بیو مکانیک گام
4.3 محدودیت
5. نتیجه گیری
تشکر و قدردانی
Abstract
1. Introduction
2. Methods
2.1. Study participants
2.2. Biomechanical analysis
2.3. Patient-reported outcome
2.4. Data reduction
2.5. Data classification
2.6. Statistical analysis
3. Results
4. Discussion
4.1. Gait biomechanics and perceived functional status
4.2. Gait biomechanics and perceived pain
4.3. Limitations
5. Conclusion
Author contributions
Declaration of interest
Acknowledgements
References