
دانلود رایگان مقاله تجزیه و تحلیل اختلال کنترل ادرار پس از رویه نوار ترا مسدودکننده
هدف: تعریف رویه نوار پس-ترامسدودکننده (پس از TOT) برای اختلال کنترل ادرار (VD) در نوشته ها ضد و نقیض است. در این مطالعه، ما با نگاهی به گذشته، عوامل ریسک پس از TOTVD را با استفاده از تعاریف مختلف در یک گروه بررسی نموده ایم.
مواد و روشها: پرونده های پزشکی 449 بیمار بعد از عمل جراحی مورد ارزیابی قرار گرفت. احتباس ادراری حاد نیازمند کاتتریزاسیون، احساس ذهنی مشکل دفع ادرار در طی پیگیری و باقی مانده پس-بعد از عمل پس از دفع ادرار- (PVR) بیشتر از 100 میلی لیتر یا PVR بیش از 50٪ حجم تخلیه شده (PVR قابل توجه) برای تعریف VD اتخاذ شد. با این دسته بندی ها، تجزیه و تحلیل چند متغیره برای عوامل ریسک VD بعد از عمل انجام شد.
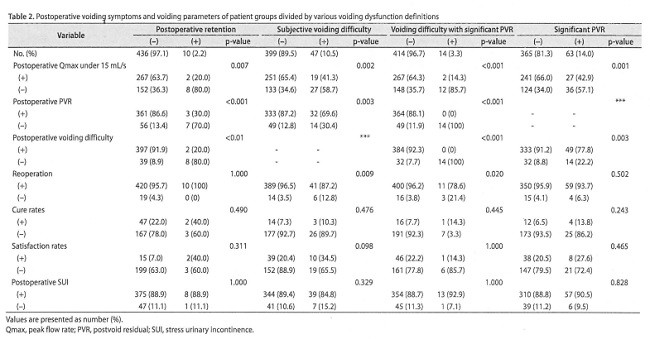
نتایج: ده بیمار (2.2٪) که به کاتتریزاسیون نیاز داشتند، 47 (10.5٪) مشکل دفع ادرار پس از عمل را تجربه کردند و 63 (14.7٪), PVR معنادار را نشان دادند. در تجزیه و تحلیل لجستیک چند متغیره، عوامل ریسک مستقل برای احتباس پس از عمل نیازمند کاتتریزاسیون, سابقه احتباس قبلی (0.06 = P) و سابقه هیسترکتومی قبل از عمل بود. عوامل ریسک برای مشکل ذهنی دفع ادرار پس از عمل, دترسور کم فعال (0.04 = P) و علائم انسدادی دفع ادرار قبل از عمل (P <0.01) بودند. تاریخ احتباس ادراری قبلی (P <0.01)) یک عامل ریسک مستقل برای مشکل ادرار کردن همزمان بعد از عمل و PVR معنی دار بود. بی حسی نخاعی ( 0.02 = p) و سابقه احتباس ادراری قبلی (P = 0.02), عوامل ریسک مستقل برای PVR قابل توجه بعد از عمل بودند.
نتیجه گیری ها: با استفاده از چندین تعریف از VD پس از رویه بند میان-مجرای ادرار، نرخ جریان پیک بعد از عمل و PVR به طور چشمگیری بین گروه های مختلف متفاوت بود. اگر چه هیچ عامل ریسک مستقل سازگار با تعاریف مختلف VD وجود نداشت، علائم انسدادی ادرار قبل از عمل و پارامترهای هدف نشاندهنده اختلال دترسور, احتمالاً دارای قدرت پیش بینی برای پس از VD TOT هستند.
مقدمه
جراحی بند میان-مجرای ادرای (MUS) غالب ترین رویه انجام شده برای درمان بی اختیاری ادرار استرسی (SUI) در زنان است. اگر چه بی اختیاری در بیشتر بیماران حل و فصل شده است، برخی از بیماران, اختلال دفع ادرار (VD) را تجربه نموده اند: که یک عارضه شایع جراحی MUS برای SUI [2] است. VD به طور بالینی نشان دهنده مشکلات دفع ادرار ذهنی و باقی مانده (PVR) و سرعت جریان کاهش یافته است.
در نوشته ها، VD بعد از عمل جراحی MUS نشان دهنده طیف گسترده ای از مشکلات دفع ادرار پس از عمل است. در یک مطالعه, VD پس از-MUS تحت معیارهای دقیق تعریف شده به عنوان نیاز برای کاتتریزاسیون مجرای اداری برای حداقل 3 روز [3] بررسی شد. دیگر نویسندگان, VD پس از MUS را به عنوان مشکل دفع ادرار گذرا تعریف نمودند که شامل مشکل دفع ادرار ذهنی و یا یک الگوی زور زدن [4[ می شود, اگرچه VD, یک عارضه به خوبی سازمان یافته است، معیار روشنی برای تعریف VD وجود ندارد.
علائم VD ممکن است در نوع و شدت در یک محدوده بین احساس تخلیه ناقص و احتباس ادرار طولانی مدت متغیر باشند. تعریف VD شامل نیاز به عمل مجدد می شود، احتباس ادراری حاد که نیاز به کاتتریزاسیون زودگذر و علایم ذهنی با یا بدون پارامترهای دفع ادرار هدف دارد [ 5]. ناراحتی ذهنی از تخلیه توسط یک جریان کاهش یافته و یا تخلیه ناقص نشان داده می شود. پارامترهای دفع ادرار هدف شامل PVR قابل توجهی با میزان جریان ادرار کاهش یافته می شود (که توسط جریان سنجی ادرار ارزیابی می شود). نیاز به یک روش اضافی برای تخلیه مثانه پس از حذف، مجرای ادرار کاتتر نیز به عنوان VD پس ازMUS [6،7] در نظر گرفته شده است.
بروز VD متغیر است و مقایسه آن با توجه به روش ها و تعاریف VD مختلف دشوار است. مداخله جراحی برای VD و حفظ ادراری در 0% تا 5 درصد از بیماران تحت عمل رویه MUS گزارش شده است [8[. مشکلات ادرار کردن بعد از عمل به مدت طولانی تر از 4 هفته در 3٪ تا 7٪ از بیماران تحت عمل های Burch [8] رخ می دهد. بنابراین، به نظر می رسد عوامل خطر VD پس ازMUS به پارامترهای متنوعی مرتبط باشد [6]. علاوه بر این، تعاریف مختلف VD پس از MUS می تواند سردرگمی در طول توضیح رضایت آگاهانه و نحوه مدیریت VD بعد از عمل را موجب شود. چنین سردرگمی می تواند منجر شود که یک پزشک از شکایت بیمار چشم پوشی نماید و یا در مورد خطر بعد از عمل VD غلو نماید [9]. بنابراین، تجزیه و تحلیل عوامل خطر VD پس از MUS با استفاده از تعاریف مختلف برای VD اهمیت دارد.
در عصر MUS، روش ها جراحی به منظور بهبود نتایج عمل جراحی و کاهش عوارض تکامل یافته اند. تعاریف و روش ها برای ارزیابی VD هنوز مورد بحث است، با این حال. در این مطالعه، ما به صورت گذشته نگر بیماران در یک گروه تک سازمانی را به منظور بررسی بروز و عوامل ریسک VD پس از عمل نوار transobturator (TOT) با استفاده از معیارهای مختلف برای VD تحلیل می کنیم.
مواد و روش ها
از ژوئن 2006 تا دسامبر 2014، در مجموع 467 بیمار در یک موسسه تک تحت عمل جراحی MUS ترانس واژینال قرار گرفتند. به استثنای موارد عمل جراحی برای برای عوارض مرتبط با MUS, سوابق پزشکی 449 نفر از گذشته مورد بررسی قرار گرفت. علائم ادرار کردن قبل و بعد از عمل از گذشته تا به حال مورد بررسی قرار گرفت. علایم دفع با گرفتن شرح حال و گزارش بیمار مورد بررسی قرار گرفت. علایم دفع انسدادی شامل جریان آهسته، تناوب، تخلیه ناقص، و تردید بود.مطالعات اورودینامیک قبل از عمل و همچنین جریان سنجی ادراری و اندازه گیری PVR انجام شد. مطالعه اورودینامیک شامل سیستومتروگرام، مطالعه فشار-جریان و اندازه گیری فشار بسته شدن مجرای ادرار و فشار نقطه نشت انجام شد. مطالعه اورودینامیک با یک سیستم اورودینامیک MMS مدل بین المللی نقره ای خورشیدی (MMS بین المللی، Dover، NH، USA) انجام شد. با استفاده از پارامترهای مطالعه جریان-فشار، ما بیماران با دترسور زیر-فعال یا انسداد خروجی مثانه زن (BOO) را متمایز نمودیم. دترسور زیر-فعال به عنوان کمتر از 20 cmH20 فشار دترسور در سرعت جریان حداکثر (pdetQmax) و کمتر از 15 میلی لیتر / ثانیه در میزان حداکثر جریان (PdetQmax) تعریف شد. BOO زن به عنوان بیش از 20 cmHp در PdetQmax و کمتر از 15 میلی لیتر / ثانیه در Qmax تعریف شد [10]. ارزیابی های خاص SUI مانند آزمون پد برای نشت ادرار، آزمون Q-Tip و، و معاینه لگنی برای پرولاپس ارگان های لگن قبل از عمل انجام شد .
عملیات TOT با بیماران تحت بی حسی نخاعی و در برخی موارد تحت بیهوشی عمومی انجام شد. Monarc Subfascial Hammock System (American Medical Systems, Minnetonka, :MN, USA) برای نوار واژن استفاده شد. تنش نوار قرار گرفته در یک حالت آزاد از تنش با در نظر گرفتن شرایط اسفنکتر و دترسور تنظیم شد. در پایان این عملیات، یک کاتتر 16-جلو Foely جایگذاری شد و روز بعد از بسیاری از بیماران برداشته شد. پس از برداشتن کاتتر مجرای ادرار، حالت ادرار بیمار با جریان سنجی ادراری ثبت شد و اندازه گیری PVR جریان سنجی ادراری در دفع ادرار دوم بعد از خروج سوند Foely ثبت شد. پارامترهای دفع ادرار و علائم آن در طول چک آپ های معمول بعد از عمل 1 هفته و 1 ماه ارزیابی شدند. حالت بی اختیاری ادراری و رضایت از عمل در 1 سال بعد از عمل مورد نظرسنجی قرار گرفتند. روش ها در مطالعه قبلی [11[شرح داده شد.
Purpose: The definition of posttransobturator tape procedure (post-TOT) voiding dysfunction (VD) is inconsistent in the literature. In this study, we retrospectively' investigated the risk factors for post-TOTVD by applying various definitions in one cohort.
Materials and Methods: The medical records of 449 patients were evaluated postoperatively. Acute urinary retention requiring catheterization, subjective feeling of voiding difficulty during follow-up, and postoperative postvoid residual (PVR) greater than 100 mL or PVR greater than 50% of voided volume (significant PVR) were adopted for the definition of VD. With these categories, multivariate analysis was performed for risk factors of postoperative VD.
Results: Ten patients (2.2%) required catheterization, 47 (10.5%) experienced postoperative voiding difficulty, and 63 (14.7%) showed significant PVR. In the multivariate logistic analysis, independent risk factors for postoperative retention requiring catheterization were previous retention history (p=0.06) and preoperative history of hysterectomy. Risk factors for subjective postoperative voiding difficulty were underactive detrusor (p=0.04) and preoperative obstructive voiding symptoms (p<O.Ol). Previous urinary retention history (p<O.Ol)) was an independent risk factor for concomitant postoperative voiding difficulty and significant PVR. Spinal anesthesia (p=0.02) and previous urinary retention history (p=0.02) were independent risk factors for significant postoperative PVR.
Conclusions: With the use of several definitions of VD after the midurethral sling procedure, postoperative peak flow rate and PVR were significantly different between groups. Although there were no independent risk factors consistent with various definitions ofVD, preoperative obstructive voiding symptoms and objective parameters suggesting impaired detrusor tend to have predictive power for post-TOT VD.
INTRODUCTION
Midurethral sling (MUS) surgery is the most frequently performed procedure to treat stress urinary incontinence (SUI) in women. Although incontinence is resolved in most patients, some patients experience voiding dysfunction (VD) [11 which is a common complication of MUS surgery for SUI [2l VD clinically represents subjective voiding difficulties and objective significant postvoid residual (PVR) and decreased flow rate. In the literature, VD after MUS surgery represents a wide spectrum of postoperative voiding problems. In one study, post-MUS VD was investigated under strict criteria defined as the need for urethral catheterization for at least 3 days [3J Other authors defined post-MUS VD as transient voiding difficulty, which included subjective voiding difficulty or a straining pattern [4J Although VD is a wellrecognized complication, there are no clear criteria to define VD.
Symptoms of VD may vary in type and severity in a range between a feeling of incomplete emptying and prolonged urinary retentioIL The definition of VD includes the need for reoperation, acute urinary retention that requires transient catheterization, and subjective symptoms with or without objective voiding parameters [5]. Subjective discomfort of emptying is represented by a reduced stream or incomplete emptying. Objective voiding parameters include significant PVR with a decreased urinary flow rate (as assessed by uroflowmetry). The need for an additional procedure for bladder emptying after urethral catheter removal is also regarded as post-MUS VD [6,7].
The incidence of VD is variable and is difficult to compare owing to the various procedures and definitions of VD. Surgical intervention for VD and urinary retention has been reported in 0"10 to 5% of patients undergoing the MUS procedure [8J Postoperative voiding difficulties lasting longer than 4 weeks occur in 3% to 7% of patients undergoing Burch procedures [8]. Therefore, the risk factors of postMUS VD appear to be related to diverse parameters [6J In addition, the various definitions of post-MUS VD can cause confusion during the explanation of informed consent and how to manage postoperative VD. Such confusion could lead a clinician to overlook the patients' complaint or overstate the risk of postoperative VD [9J Thus, it is meaningful to analyze the risk factors for post-MUS VD with the use of various definitions for VD.
In the MUS era, surgery methods have evolved to improve the results of surgery and decrease the complications. The definitions of and methods for evaluating VD are still controversial, however. In this study, we retrospectively analyzed patients in a single institutional cohort to investigate the incidence and risk factors of VD after the transobturator tape procedure (TOT) by applying various criteria for VD.
MATERIALS AND METHODS
From June 2006 to December 2014, a total of 467 patients underwent a transvaginal MUS operation for SUI at a single institutiOIL Excluding the cases of surgery for MUS. related complications, the medical records of 449 patients were reviewed retrospectively. Pre- and postoperative voiding symptoms were evaluated retrospectively. Voiding symptoms were evaluated by history taking and patient reports. Obstructive voiding symptoms included slow stream, intermittency, incomplete emptying, and hesitancy. Preoperative urodynamic studies were performed as well as uroflowmetry and measurement of PVR The urodynamic study included cystometrogram, pressure-flow study, and Pleasurement of urethral closure pressure and leak point pressure. The urodynamic study was performed with an MMS International model solar silver urodynamic system (MMS International, Dover, NH, USA). By use of pressureflow study parameters, we discriminated between patients with an underactive detrusor or female bladder outlet obstruction (BOO). Underactive detrusor was defined as less than 20 cmH20 in detrusor pressure at maximal flow rate (pdetQmax) and less than 15 mL/s in peak flow rate (Qmax). Female BOO was defined as more than 20 cmHp in PdetQmax and less than 15 mL/s in Qmax [10J Specific evaluations of SUI such as the pad test for urine leakage, Q-tip test, and pelvic examination for pelvic organ prolapse were performed preoperatively.
The TOT operation was performed with the patients under spinal anesthesia and in some cases under general anesthesia. The Monarc Subfascial Hammock System (American Medical Systems, Minnetonka, :MN, USA) was used for the vaginal tape. The tension of the indwelled tape was adjusted to a tension-free state taking into account the condition of the sphincter and detrusor. At the end of the operation, a 16-Fr Foley catheter was indwelled and was removed the next day in most patients. After removal of the urethral catheter, the patients' voiding state was recorded with uroflowmetry and measurement of PVR Uroflowmetry was performed at the second voiding after Foley catheter removal Voiding parameters and voiding symptoms were evaluated during routine check-ups at postoperative 1 week and 1 month. Incontinence state and satisfaction with the operation were surveyed at postoperative 1 year. The procedures were described in a previous study [11l.
مقدمه
مواد و روش ها
نتایج
بررسی
نتایج
INTRODUCTION
Materials and Methods
Results
DISCUSSION
Conclusions
CONFLICTS OF INTEREST