
دانلود رایگان مقاله پیوستگی علائم افسردگی قبل و بعد از تشخیص یک بیماری مزمن
چکیده
پیشینه: بسیاری از بیماری های مزمن ، خطر ابتلا به علائم افسردگی را افزایش می دهند، اما مطالعات کمی در مورد اینکه آیا این بیماری ها بر ترکیب علائمی که احتمالا فرد تجربه کرده است نیز تاثیر دارد، مورد بررسی قرار گرفته است. از آنجایی که خطر ابتلا و پیشرفت افسردگی ممکن است بین بیماریهای مزمن متفاوت باشد، ما از تحلیل شبکه ای برای بررسی چگونگی پیوستگی علائم افسردگی قبل و بعد از تشخیص دیابت، بیماری های قلبی، سکته و سرطان استفاده کردیم.
روش کار: شرکت کنندگان (N=7779) از نظرسنجی طولی مطالعه سلامت و بازنشستگی بودند. شرکت کنندگان در صورتی واجد شرایط بودند که علائم افسردگی را دو یا چهار سال قبل و بعد از تشخیص دیابت، بیماری های قلبی، سرطان یا سکته داشته باشند. ما یک گروه کنترل بدون بیماری مزمن تشکیل دادیم که از نظر سن، جنس و پیشینه نژادی با افراد مبتلا به این بیماری مطابقت داشته باشد. شبکه های علائم افسردگی را ایجاد کردیم و پیوستگی کلی آن شبکه ها و نمرات مجموع علائم افسردگی را برای قبل و بعد از تشخیص هر بیماری مورد مقایسه قرار دادیم.
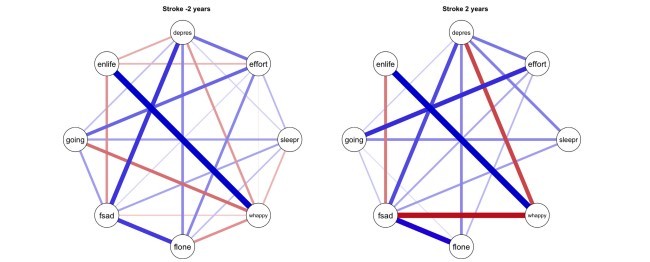
نتایج: نمرات مجموع علائم افسردگی با تشخیص هر بیماری افزایش یافت. پیوستگی علائم افسردگی برای تمام بیماری ها به جز سکته بدون تغییر باقی ماند که در این مورد پیوستگی با تشخیص کاهش پیدا کرد.
محدودیت ها: همبودی با سایر بیماری های مزمن کنترل نشده بود، زیرا ما بر بروز بیماری های خاص تمرکز کردیم.
نتیجه گیری: نتایج ما نشان می دهد که اگرچه سطح متوسط علائم افسردگی بعد از تشخیص بیماری مزمن افزایش می یابد، اما در بیشتر بیماری های مزمن، این تغییرات در ساختار شبکه ای علائم افسردگی منعکس نمی-شوند.
1. مقدمه
افسردگی نوعی اختلال روانپزشکی ناهمگن است که اغلب با بیماری های دیگر همراه است (راش و راش، 2007). به نظر می رسد که این ارتباط ها دو طرفه هستند: افراد مبتلا به افسردگی در معرض خطر ابتلا به چندین بیماری مزمن مانند دیابت، بیماری های قلبی و عروقی، سرطان و سکته قرار دارند (اوتزنایدر و همکاران، 2007؛ شین و همکاران، علی و همکاران، 2006؛ ویلیامز و همکاران، 2004؛ اندرسون و همکاران، 2001، موسوی و همکاران، 2007)، اما بیماری های مزمن ممکن است در بروز افسردگی نیز نقش داشته باشند (علی و همکاران، 2006؛ اندرسون و همکاران، 2001؛ هاکت و اندرسون، 2005)، زیرا سازگاری روانشناختی با بیماری های مزمن می تواند بسیار چالش برانگیز باشد (دریدر و همکاران، 2008). علاوه بر این، مطالعات نشان می دهد که وقوع بیماری مزمن و افسردگی باعث بدتر شدن سلامتی در مقایسه با داشتن یک بیماری به تنهایی شود (موسوی و همکاران، 2007) و چنین رویدادی با افزایش مرگ و میر همراه بوده است (ویلیامز و همکاران، 2004؛ پینکارت و دوبرشتین، 2010). افسردگی شامل علائم مختلفی از جمله، کج خلقی، اختلال در خواب، تنهایی، عدم ابتکار و فقدان لذت می شود. با این وجود، مشخص نیست که آیا الگوی علائم بسته به وضعیت بیماری جسمی متفاوت است یا خیر.
شدت افسردگی با شمارش تعداد علائم افسردگی برای یک فرد خاص اندازه گیری شده است (تشخیصی و آماری، 2013)، اما گفته می شود که چنین مقیاس کلی ممکن است به اندازه کافی پیچیدگی افسردگی را نشان ندهد (فرید و نسی، 2015). یک روش جایگزین بررسی ساختار شبکه و پویایی علائم افسردگی خاص است، یعنی اینکه چگونه علائم به هم متصل هستند. برای مثال، شبکه ای متراکم تر و محکم تر ممکن است خطر بیشتری برای ابتلا به افسردگی را نشان دهد (کرامر و همکاران، 2016). همچنین یک ساختار شبکه ای به شدت مرتبط با علائم افسردگی، افسردگی پایدار را در مقایسه با افسردگی ناپایدار نشان داده است (ون بورکولو و همکاران، 2015). ساختار شبکه ای علائم افسردگی نیز ممکن است نسبت به تغییرات در سلامت جسمی حساس باشد.
در این مطالعه، چگونگی ارتباط علائم افسردگی قبل و بعد از تشخیص بیماری مزمن شایع بررسی شده است. از آنجایی که الگوی علائم می تواند مختص بیماری های جسمی باشد، ما بر روی چندین بیماری مزمن شایع از جمله دیابت، بیماری قلبی و عروقی، سکته و سرطان تمرکز کردیم. برای هر بیماری، ما شبکه های علائم افسردگی را قبل و بعد از تشخیص تعیین کردیم و چگونگی پیوستگی کلی آن شبکه ها را در مقایسه با اندازه گیری سنتی نمره مجموع مقیاس افسردگی مقایسه کردیم. براساس یافته های مطالعات قبلی (کرامر و همکاران، 2016؛ ون بورکولو و همکاران، 2015) فرض کردیم که پیوستگی کلی شبکه های علائم افسردگی پس از تشخیص بیماری مزمن افزایش می یابد.
2. روش ها
2.1. طرح مطالعه و شرکت کنندگان
شرکت کنندگان در این مطالعه از مطالعه سلامت و بازنشستگی (HRS)(سونگا و همکاران، 2014) بودند. HRS یک نظرسنجی طولی در سطح ملی از افراد بالای پنجاه سال در آمریکا است که در سال 1992 آغاز شد. این تحقیق هر دو سال یکبار انجام می شود. موج اول شامل معیار علائم افسردگی است، اما نسخه ای است که 11 مورد را با مقیاس واکنش 4 نقطه ای مشخص می کند، در حالی که تمام موج های دیگر از یک معیار علائم افسردگی استفاده می کنند که شامل 8 مورد با مقیاس واکنش 2 نقطه ای است. نشان داده شده است که این معیارها با هم اختلاف دارند و تجزیه و تحلیل موج متقابل توصیه نمی شود (استیفیک، 2000). بنابراین، امواج نظرسنجی از سال 1994 تا 2014 در این مطالعه استفاده شده است.
شرکت کنندگان در صورتی واجد شرایط بودند که علائم افسردگی را دو یا چهار سال قبل و بعد از تشخیص دیابت، بیماری های قلبی، سرطان یا سکته داشته باشند. به همراه یک گروه کنترل که هیچ بیماری نداشت، مطالعه ما شامل 7779 مرد و زن بود. HRS مورد تایید هیئت بازنگری نهادی دانشگاه میشیگان قرار گرفته است و این مطالعه طبق اصول اعلامیه هلسینگی انجام شده است. HRS با جزئیات بیشتری در جای دیگر توصیف شده است (سونگا و همکاران، 2014).
2.2. اندازه گیری علائم افسردگی
علائم افسردگی با استفاده از مرکز مطالعات اپیدمیولوژیک افسردگی (CES-D) اندازه گیری شد (رادلوف، 1977). این مقیاس شامل هشت شاخص برای افسردگی است: احساس افسردگی، همه چیز با تلاش است، خواب بی قرار، احساس تنهایی، احساس غم، احساس می کند نمی تواند به زندگی ادامه دهد، خوشحال باشد و از زندگی لذت ببرد. پاسخ به هر شاخص به صورت بله یا خیر است. نمره خلاصه برای مقیاس جمع بندی تمام پاسخ ها برای هر شرکت کننده محاسبه شد. پاسخ برای شاخص های "احساس خوشحالی" و "لذت بردن از زندگی" برای نمره خلاصه معکوس شدند.
2.3. بیماری های مزمن
در هر موج از شرکت کنندگان سؤال شد که آیا پزشک به آنها گفته بود که یکی از این شرایط زیر را داشته اند: 1) دیابت یا قند خون بالا، 2) حمله قلبی، بیماری قلبی عروقی، گلو درد، نارسایی قلبی یا سایر مشکلات قلبی، 3) سرطان یا تومور بدخیم از هر نوع به جز سرطان پوست، یا 4) سکته یا حمله ایسکمیک گذرا. هنگامی که شرکت کنندگان برای اولین بار گزارش دادند که به یک بیماری مبتلا شده اند، موج سال صفر کدگذاری شد. دو موج قبل به صورت -2 و -4، و دو موج متوالی به عنوان 2 و 4 کدگذاری شده بودند.
ABSTRACT
Background: Many chronic diseases increase the risk of depressive symptoms, but few studies have examined whether these diseases also affect the composition of symptoms a person is likely to experience. As the risk and progression of depression may vary between chronic diseases, we used network analysis to examine how depression symptoms are connected before and after the diagnosis of diabetes, heart disease, stroke, and cancer.
Methods: Participants (N = 7779) were from the longitudinal survey of the Health and Retirement Study. Participants were eligible if they had information on depression symptoms two and/or four years before and after the diagnosis of either diabetes, heart disease, cancer or stroke. We formed a control group with no chronic disease that was matched on age, sex and ethnic background to those with a disease. We constructed depression symptom networks and compared the overall connectivity of those networks, and depression symptom sum scores, for before and after the diagnosis of each disease.
Results: Depression symptom sum scores increased with the diagnosis of each disease. The connectivity of depression symptoms remained unchanged for all the diseases, except for stroke, for which the connectivity decreased with the diagnosis.
Limitations: Comorbidity with other chronic diseases was not controlled for as we focused on the onset of specific diseases.
Conclusions: Our results suggest that although the mean level of depression symptoms increases after the diagnosis of chronic disease, with most chronic diseases, these changes are not reflected in the network structure of depression symptoms.
1. Introduction
Depression is a heterogeneous psychiatric disorder that is often associated with other diseases (Rush and Rush, 2007). These associations also appear to be bidirectional: people with depression have an increased risk of several chronic conditions, such as diabetes, cardiovascular disease, cancer, and stroke (Utzschneider et al., 2007, Schane et al., Ali et al., 2006, Williams et al., 2004, Anderson et al., 2001, Moussavi et al., 2007), but chronic diseases may also contribute to onset of depression (Ali et al., 2006, Anderson et al., 2001, Hackett and Anderson, 2005), as the psychological adjustment to chronic illnesses can be highly challenging (de Ridder et al., 2008). In addition, studies suggest that the co-occurrence of chronic disease and depression may incremental worsen health compared to having either disease alone (Moussavi et al., 2007), and such co-occurrence has been associated with increased mortality (Williams et al., 2004, Pinquart and Duberstein, 2010). Depression involves several symptoms, including e.g. low mood, sleep disturbance, loneliness, lack of initiative, and anhedonia. However, little is known whether the pattern of symptoms might vary depending on the status of physical disease.
The severity of depression has been measured by counting how many depression symptoms are present for a given individual (Diagnostic and Statistical 2013), but it has been argued that such an aggregate measure might not adequately portray the complexity of depression (Fried and Nesse, 2015). An alternative approach is to examine the network structure and dynamics of specific depression symptoms, that is, how the symptoms are connected. A denser, more tightly knit network of symptoms, for example, may indicate a higher risk for developing depression (Cramer et al., 2016). A more strongly connected network structure of depression symptoms has also been shown to characterize persistent depression compared to more transient depression (Van Borkulo et al., 2015). The network structure of depression symptoms might also be sensitive to changes in physical health.
In this study, we examined how depression symptoms were connected before and after the diagnosis of common chronic illness. As the pattern of symptoms can be specific to physical disease, we focused on multiple common chronic illnesses, including diabetes, coronary heart disease, stroke, and cancer. For each disease, we determined depression symptom networks before and after the diagnosis and examined how the overall connectivity of those networks compared against the traditional measure of depression scale sum score. Based on the findings from previous studies (Cramer et al., 2016, Van Borkulo et al., 2015) we hypothesized that the overall connectivity of depression symptom networks increases after the diagnosis of a chronic illness.
2. Methods
2.1. Study design and participants
The participants for this study were from the Health and Retirement Study (HRS) (Sonnega et al., 2014). HRS is a nationally representative longitudinal survey of people over age 50 in the USA that started in 1992. The survey is conducted every two years. The first wave includes a measure of depressive symptoms, but it is a version that features 11 items with a 4-point response scale, whereas all the other waves use a measure of depressive symptoms which includes 8 items with a 2-point response scale. The measures have been shown to be in disagreement and cross-wave analysis is not recommended (Steffick, 2000). Therefore, survey waves from 1994 to 2014 were used in this study.
Participants were eligible for this study if they had information on depression symptoms two and/or four years before and after the diagnosis of either diabetes, heart disease, cancer or stroke. Together with a control group that had none of the illnesses, our study included 7779 men and women.
HRS has been approved by the University of Michigan Institutional Review Board, and the study has been conducted according to the principles of the Declaration of Helsinki. HRS is described in more detail elsewhere (Sonnega et al., 2014).
2.2. Measurement of depression symptoms
Depression symptoms were measured using the Center for Epidemiologic Studies Depression (CES-D) scale (Radloff, 1977). The scale consists of eight indicators for depression: felt depressed, everything is an effort, sleep is restless, felt alone, felt sad, and could not get going, felt happy, and enjoyed life. Responses for each indicator were given as either yes or no. A summary score for the scale was computed for each participant by summing together all the answers. The answers for indicators “felt happy” and “enjoyed life” were reversed for the summary score.
2.3. Chronic diseases
In each wave, participants were asked whether a doctor had told them if they had one of the following conditions: 1) diabetes or high blood sugar, 2) heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems, 3) cancer or a malignant tumor of any kind except skin cancer, or 4) stroke or transient ischemic attack. The wave when participants first reported having been diagnosed with a disease was coded as year zero. The preceding two waves were coded as -2 and -4, and the two successive waves as 2 and 4.
چکیده
1. مقدمه
2. روش ها
2.1. طرح مطالعه و شرکت کنندگان
2.2. اندازه گیری علائم افسردگی
2.3. بیماری های مزمن
2.4. گروه کنترل
2.5. تحلیل آماری
3. نتایج
4. بحث
4.1. محدودیت ها
5. نتیجه گیری
منابع
ABSTRACT
1. Introduction
2. Methods
2.1. Study design and participants
2.2. Measurement of depression symptoms
2.3. Chronic diseases
2.4. Control group
2.5. Statistical analysis
3. Results
4. Discussion
4.1. Limitations
5. Conclusions
References