
دانلود رایگان مقاله به روز رسانی مدیریت یبوست در سالمندان
خلاصه:
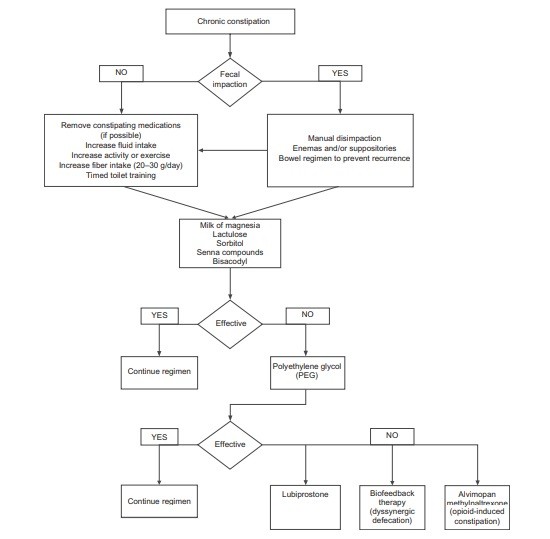
یبوست به طور نامتناسبی بر افراد مسن تاثیر می گذارد، با شیوع 50 درصد، در جامعه سالمندان و 74٪ در ساکنین خانه سالمندان. از دست دادن تحرک، داروها، بیماری های زمینه ای، اختلال در حس مقعد، و نادیده گرفتن تماس برای اجابت مزاج به اندازه دفع مدفوع dyssynergic یا سندرم روده تحریک پذیر که باعث یبوست می شوند، مهم است. تاریخ دقیق پزشکی در مورد داروها و مشکلات بیماری، و معاینه دقیق رکتال دیجیتال ممکن است به شناسایی علل یبوست کمک کند. به همین ترتیب، آزمایش خون و کولونوسکوپی ممکن است به شناسایی علل ارگانیک مانند سرطان روده بزرگ کمک کند. تست های روانشناسی مانند مطالعه ترانزیت کولون با نشانگر رادیویی مات و یا کپسول تحرک بی سیم، مانومتری آنورکتال و آزمون های اخراج بالون می تواند اختلالات عملکرد کولون و مقعد را تشخیص دهد. با این حال، در افراد مسن، معمولا بیش از یک مکانیزم وجود دارد که نیاز به یک رویکرد درمان فردی و در عین حال عاملی دارد. مدیریت یبوست به تکامل خود ادامه میدهد. اگر چه مسهل های اسموتیک مانند پلی اتیلن گلیکول به عنوان مهار اصلی باقی می ماند، به نظر می رسد چند عوامل جدید که مکانیزم های مختلف را هدف قرار می دهند، مانند کلرید کانال فعال (lubiprostone) guanylate آگونیست سیکلاز (linaclotide)، آگونیست 5HT4 (prucalopride)، و آنتاگونیست های گیرنده محیطی μ عمل کننده (alvimopan و methylnaltrexone) برای یبوست ناشی از مواد مخدر مفید باشند. درمان بیو فیدبک برای دفع مدفوع dyssynergic و مدفوعی با کثیف کردن موثر است. با این حال، داده ها در مورد اثر بخشی و ایمنی مواد مخدر در افراد مسن، محدود و ضروری و مورد نیاز هستند.
مقدمه
مدیریت یبوست در سالمندان در حال به چالش کشیدن بیماران و ارائه دهندگان خدمات درمانی است. دلایل متعدد منجر به این پدیده وجود دارد، مانند اثر گذشت زمان بر فیزیولوژی دستگاه گوارش، بیماری مشترک و مرضی، داروها، از دست دادن تحرک، مصرف کالری ناکافی و تغییرات حسی مقعد. بیماران مسن، به خصوص کسانی که مبتلا به زوال عقل پیشرفته در خانه های سالمندان هستند و کسانی که بر روی شبه افیونی ها برای تسکین دهنده مراقبت از خود کار می کنند، نیاز به یک رویکرد منحصر به فرد برای درمان یبوست دارند.
تعریف و اپیدمیولوژی
یبوست یک مقوله بیماری به خوبی تعریف نیست، بلکه یک اصطلاح عمومی برای توصیف مشکلاتی است که یک فرد با حرکت روده خود تجربه می کند. ارائه دهندگان بهداشت و درمان به طور معمول یبوست را به عنوان فراوانی مدفوع کمتر از 3 حرکت در هفته تعریف می کنند. در مقابل، بیماران مشکل یبوست به عنوان هر نوع از اجابت مزاج، از جمله زور زدن، مدفوع سخت، احساس دفع ناکامل، و خلط تعریف می کنند. در مقایسه با بیماران جوانتر، این گزارش زور زدن شایع تر افراد مسن، خود انشعاب پنجه، و احساسات بسته شدن مقعد را گزارش می دهد. در یک مطالعه از 531 بیمار در عمل به طور کلی، 50٪ تعریف های مختلفی را از یبوست در مقایسه با پزشکان خود ارائه دادند. به علت این تعاریف متغیر از یبوست، یک پانل بین المللی از کارشناسان مشخصه رم Rome criteria را برای یبوست پیشنهاد دادند. معیارهای استفاده شده III Rome از ترکیبی از علائم ذهنی برای تعریف یبوست استفاده نمودند و در حال حاضر به طور گسترده ای برای انجام تحقیقات بالینی در این زمینه استفاده می شوند.
گزارش شده است که شیوع یبوست با سن افزایش می یابد، به ویژه افراد با بیش از سن از 65 سال. در بیماران سالمند که در جامعه زندگی می کنند، شیوع یبوست50٪ . است. این عدد در پرستاری ساکنان خانه، با 74٪ با استفاده از ضدیبوست روزانه حتی بالاتر است. به همین ترتیب، احتمال دارد زنان مسن 2 تا 3 برابر بیشتر به یبوست را نسبت به خود مردان گزارش دهند. یبوست نیز معمولا بیشتر در بیماران مصرف کننده داروهای متعدد دیده می شود.
کیفیت زندگی مرتبط با سلامت و یبوست
مدارک و شواهد در ابزارهای کیفیت بیماری خاص و عمومی زندگی (QOL) نشان داده است که یبوست با اختلال در کیفیت زندگی مرتبط با سلامت (HR-QOL) همراه است. به عنوان مثال، در یک مطالعه از 126 جامعه، بزرگسالان خانه های قدیمی تر ، افراد مبتلا به یبوست مزمن برای عملکرد جسمی، روانی بهداشت، مفهوم سلامت به طور کلی، و درد بدن نسبت به پاسخ دهندگان با هیچ یبوستی دارای امتیازات 36 Short-Form (SF-36) نمره هستند. همین ترتیب، استفاده از شاخص رفاه روانی (PGWB) ،84 نفر با یبوست دارای نمره کل کمتر PGWB و به علت اضطراب، افسردگی، خوب بودن، خود کنترلی و خرده مقیاس های سلامت عمومی دارای دامنه نمرات پایین تری بودند که HR-QOL. بدتر را نشان می دهد. علاوه بر این، بهبود با HR-QOL با درمان یبوست مشخص می شود. پس از اینکه مسهل ها افزایش قابل توجهی در اجابت مزاج را در یک هفته ایجاد نمودند، بیماران علائم ادراری کمتر، عملکرد جنسی بهتر و بهبود خلق و افسردگی را نشان دادند.
علاوه بر این، یبوست محرک قابل توجهی در هزینه های مراقبت از سلامت است، همانطور که در میان 5 تشخیص رایج رتبه بندی برای ویزیت پزشک برای بیماران سرپایی دستگاه گوارش رده بندی می شود. با استفاده از یک مطالعه جامعه، مدیریت یبوست به طور متوسط $ 200 به ازای هر بیمار در داخل یک HMO.16 بزرگ تخمین زده می شود. بیش از $ 821 میلیون دلار (2000 ارزش) برای مسهل ها در ایالات متحده به تنهایی صرف شده است. دیگر هزینه های غیر مستقیم یبوست برای جامعه عبارتند از کاهش کار بهره وری، غیبت در مدرسه، با کیفیت پایین زندگی و روانی بالاتر در اضطراب هستند.
خویشتن داری و اجابت طبیعی مزاج
کف لگن شامل عضلات سطحی و لایه هایی عمیق می شود که راست روده، مثانه و رحم را در بر می گیرد.17 لایه های سطحی عضلانی شامل اسفنکترهای مقعد داخلی و خارجی تشکیل شده، پرینه بدن و عضلات عرضی perinei. می شوند. در مقابل، عضلات عمیق لگن (که همچنین به عنوان لواتور آنی شناخته شده هستند) از pubococcygeus، ileococcygeus و ماهیچه های puborectalis.17 تشکیل می شوند. این ساختار تا حد زیادی به عصب ریشه های عصبی خاجی (S2-S4) و عصب pudendalمرتبط می شود.
خویشتن داری، توانایی برای حفظ مدفوع است تا زمانی که به لحاظ اجتماعی منجر به دفع شود، در حالی که دفع مدفوع، تخلیه مواد دفعی از روده بزرگ است. هر دو توابع با ساز و کارهای داوطلبانه و غیر ارادی رفلکس، آناتومیک عوامل، احساس رکتوم، و پیروی از رکتوم تنظیم می شوند.
دفع مدفوع زمانی شروع می شود که قشر مخ آگاهی و درک از سطح بحرانی پر کردن را در مقعد دریافت می کند. هنگامی که فرد نشستن و یا چمباتمه زدن را تطبیق می دهد، اسفنکترهای مقعد و puborectalis ارام می گیرند و زاویه مقعد را صاف می کنند. همزمان، تلاش داوطلبانه برای تحمل کردن فشار داخل شکمی را افزایش می دهد که موجب تسهیل توسعه یک موج سلب و در نتیجه تخلیه مدفوع می شود.
Abstract:
Constipation disproportionately affects older adults, with a prevalences of 50% in community-dwelling elderly and 74% in nursing-home residents. Loss of mobility, medications, underlying diseases, impaired anorectal sensation, and ignoring calls to defecate are as important as dyssynergic defecation or irritable bowel syndrome in causing constipation. Detailed medical history on medications and co-morbid problems, and meticulous digital rectal examination may help identify causes of constipation. Likewise, blood tests and colonoscopy may identify organic causes such as colon cancer. Physiological tests such as colonic transit study with radio-opaque markers or wireless motility capsule, anorectal manometry, and balloon expulsion tests can identify disorders of colonic and anorectal function. However, in the elderly, there is usually more than one mechanism, requiring an individualized but multifactorial treatment approach. The management of constipation continues to evolve. Although osmotic laxatives such as polyethylene glycol remain mainstay, several new agents that target different mechanisms appear promising such as chloride-channel activator (lubiprostone), guanylate cyclase agonist (linaclotide), 5HT4 agonist (prucalopride), and peripherally acting µ-opioid receptor antagonists (alvimopan and methylnaltrexone) for opioid-induced constipation. Biofeedback therapy is efficacious for treating dyssynergic defecation and fecal impaction with soiling. However, data on efficacy and safety of drugs in elderly are limited and urgently needed.
Introduction
The management of constipation in the elderly is challenging both for patients and healthcare providers. Multiple reasons contribute to this phenomenon, such as the effects of aging on gut physiology, co-morbid illnesses, medications, loss of mobility, inadequate caloric intake, and anorectal sensory changes. Elderly patients, especially those with advanced dementia in nursing homes and those on opioids for palliative care, require an individualized approach for the treatment of constipation.
Definition and epidemiology
Constipation is not a well defined disease entity, but a general term used to describe the difficulties that a subject experiences with moving their bowels.1 Healthcare providers typically define constipation as stool frequency of less than 3 bowel movements per week.2 In contrast, patients define constipation as any form of “difficult defecation”, such as straining, hard stool, feeling of incomplete evacuation, and nonproductive urge.3,4 Compared to younger patients, the elderly report more frequent straining, self-digitation, and feelings of anal blockage.4,5 In a study of 531 patients in general practice, 50% gave a different definition of constipation compared to their physicians.6 Because of these variable definitions of constipation, an international panel of experts proposed the Rome criteria for constipation. The Rome III criteria used a combination of subjective symptoms to define constipation,7 and are currently used widely for performing clinical research in this field.
It is reported that the prevalence of constipation increases with age, especially those over the age of 65 years.8 In elderly patients living in the community, the prevalence of constipation is 50%.4 This number is even higher in nursing home residents, with 74% using daily laxatives.4,9–11 Likewise, elderly women are 2 to 3 times more likely to report constipation than their male counterparts.4 Constipation is also more commonly seen in patients taking multiple medications.12
Health-related quality of life and constipation
Evidence in both disease-specific and generic quality of life (QOL) instruments has shown that constipation is associated with impaired health-related quality of life (HR-QOL). For example, in one study of 126 community-dwelling older adults, respondents with chronic constipation had lower Short-Form 36 (SF-36) scores for physical functioning, mental health, general health perception, and bodily pain when compared to respondents with no constipation.13 Likewise, using the Psychological General Well-Being (PGWB) index, 84 subjects with constipation has lower PGWB total scores and lower domain scores for anxiety, depression, well-being, self-control and general health subscales, indicating worse HR-QOL.14 Furthermore, improvements with HR-QOL were noted with treatment of constipation.15 After laxatives caused significant increases in weekly bowel movements, patients reported fewer urinary symptoms, better sexual function and improved mood and depression.
In addition, constipation is a significant driver of health care costs, as it is ranked among the top 5 most common physician diagnosis for gastrointestinal outpatient visits.4 Using a community survey, the management of constipation is estimated to average $200 per patient within a large HMO.16 Over $821 million dollars (2000 value) was spent on over-the-counter laxatives in the United States alone.8 Other indirect costs of constipation to society include decrease in work related productivity, absences in school, lower quality of life and higher psychological distress.
Normal continence and defecation
The pelvic floor consists of superficial and deep muscle layers that envelope the rectum, bladder and uterus.17 The superficial muscle layers consist of the internal and external anal sphincters, the perineal body and the transverse perinei muscles. In contrast, the deep pelvic muscles (also known as levator ani) are composed of the pubococcygeus, ileococcygeus and puborectalis muscles.17 These structures are largely innervated by the sacral nerve roots (S2 –S4 ) and the pudendal nerve.
Continence is the ability to retain feces until it is socially conducive to defecate, while defecation is the evacuation of fecal material from the colon. Both functions are regulated by voluntary and involuntary reflex mechanisms, anatomic factors, rectal sensation, and rectal compliance.
Defecation starts when the cerebral cortex receives an awareness and perception of critical level of filling in the rectum. When the individual adopts a sitting or squatting position, the anal sphincters and the puborectalis relax, straightening the anorectal angle. Simultaneously, the voluntary efforts of bearing down increases the intra-abdominal pressure, facilitating the development of a stripping wave, resulting in stool evacuation.
چکیده
مقدمه
اجابت مزاج Dyssynergic
تشخیص یبوست در افراد مسن
تاریخچه پزشکی و معاینه فیزیکی
ارزیابی متابولیک و ساختاری
تست های روانشناسی
مانومتری آنورکتال
آزمون اخراج بالون
مصرف مایعات و ورزش، مصرف کالری و آموزش آداب دستشویی رفتن بهنگام
رژیم غذایی و فیبر
مسهل ها
نرم کننده های مدفوع، شیاف و انما
گزینه های درمانی جدیدتر و آتی
Lubiprostone
Prucalopride
Linaclotide
کلشی سین
اجابت مزاج Dyssynergic و مدفوعی با لکه دار کردن
عمل جراحی
خلاصه
Abstract
Introduction
Definition and epidemiology
Health-related quality of life and constipation
Normal continence and defecation
Common causes of constipation in the elderly
Disorders of colonic and anorectal function causing constipation in the elderly
Slow transit constipation
Dyssynergic defecation
Irritable bowel syndrome with constipation
Diagnosis of constipation in the elderly
Metabolic and structural evaluation
Physiological tests
Colonic transit study
Anorectal manometry
Balloon expulsion test
Prevention and management of constipation in the elderly
Fluid intake and exercise, caloric intake and timed toilet training
Diet and fiber
Laxatives
Stool softeners, suppositories and enemas
Newer and upcoming treatment options
Lubiprostone
Prucalopride
Linaclotide
Colchicine
Alvimopan and methylnaltrexone
Dyssynergic defecation and fecal impaction with soiling
Surgery
Summary
Disclosures