
دانلود رایگان مقاله دیدگاه های کارکنان بهداشت و درمان در مورد کار تیمی بین حرفه ای
چکیده
کار تیمی چند تخصصی موثر نقش مهمی در پاسخگویی موفق به بحران دارد. پاسخ به بحران های بهداشت عمومی گذشته بر ارتباطات چند تخصصی و اعتماد برای حمایت از تاب آوری کارکنان بهداشت و درمان (HCW) متکی بوده است. برای درک تعاملات بین حرفه ای و درک کار تیمی در طول پاسخ کووید-19، ما مصاحبه های نیمه ساختاریافته عمیقی را با 18 HCW بستری (11 پرستار کنار تخت، 5 هماهنگ کننده مراقبت و 2 داروساز) از یک مرکز پزشکی VA بین مارس و ژوئن 2020 انجام دادیم. با استفاده از تجزیه و تحلیل موضوعی، ما چهار موضوع کلیدی را شناسایی کردیم که نقاط قوت و چالش های کار تیمی بین حرفه ای، ارتباطات، مراقبت از بیمار، و پاسخ سازمانی را در طول موج اولیه کووید-19 توصیف می کند. تیم های بین حرفه ای تکه تکه شدند. HCW هایی که به کار از راه دور منتقل شدند وضعیت خود را در تیم های بستری از دست دادند و برای ارائه سطوح کیفیت مراقبت قبل از همه گیری تلاش کردند. برعکس، کار تیمی بین حرفه ای برای HCW هایی که به کار در واحدهای بستری ادامه دادند، بهبود یافت، جایی که شرکت کنندگان در مطالعه کاهش سلسله مراتب بین حرفه ای و افزایش حمایت متقابل را توصیف کردند. شرکت کنندگان نیاز به ارتباطات به موقع، دقیق و شفاف را به دلیل مواجهه با چالش های جدید ایمنی بیمار و ارتباطات ناشی از بیماری همه گیر توصیف کردند. HCW ها تمایل خود را برای حمایت رهبری پایدار و شمول در تصمیم گیری سازمانی ابراز کردند. چالشهای کار تیمی، ارتباطات و مراقبت از بیمار گزارششده در این مطالعه، نیاز به ارتباطات منسجم، شفاف و پاسخ سازمانی از سوی رهبری بیمارستان در زمانهای بحران را برجسته میکند.
1. مقدمه
در طول همهگیری کووید-19، کارکنان بهداشت و درمان (HCW) در بیمارستانها با استرسهای حرفهای و شخصی قابلتوجهی مواجه شدهاند که منجر به ترک کار و آسیب اخلاقی شده است. آنها با تامین ناکافی تجهیزات حفاظت فردی، اضطراب در مورد انتشار ویروس به عزیزان، و نگرانی در مورد پروتکلها، رویهها و استانداردهای عمل بستری در حال تغییر سریع مبارزه کردهاند. 1،2 همکاری چند تخصصی یک عامل کلیدی در ایمنی بیمار و ارتباط موفق است. بهویژه در طول همهگیری کووید-19، بهعنوان کار گروهی مؤثر برای حمایت از HCW در طول پاسخ به بحران های گذشته ضروری بوده است.
میزان استرس، اضطراب و افسردگی در میان پاسخ دهندگان خط مقدم بالا است،5 و کار در طول کووید-19 منجر به خستگی مزمن، بی خوابی، PTSD و فرسودگی شغلی در میان متخصصان بهداشت و درمان شده است. نقش بسزایی در توانمندسازی کارکنان و سلامت فردی دارند. در طول شیوع سندرم تنفسی حاد شدید در سال 2003 و شیوع سندرم تنفسی خاورمیانه در سال 2012، ارتباط موثر، همکاری و اعتماد بین تیم های ارائه دهنده بهداشت و درمان برای مدیریت بحران بسیار مهم بود. این احساس نزدیکی و توانمندی را ایجاد کرد که به نوبه خود رهبری جمعی قوی و انعطافپذیری کارکنان را تقویت کرد. 7،8 HCW که در طول همهگیری آنفلوانزای H1N1 در سال 2009 و پاسخ بیماری ویروس ابولا در سال 2014 کار میکردند، اهمیت دریافت آموزش کار تیمی و ایجاد را توصیف کردند. شفافیت در مورد نقش های تیم برای حمایت از ایمنی بیمار و سلامت شخصی، و به این موضوع به عنوان یک زمینه کلیدی برای آمادگی برای شیوع بیماری های آینده اشاره کرد.
در طول همهگیری کنونی کووید-19، چندین سیستم بیمارستانی موفق شدند تیمهای چند تخصصی خط مقدم را برای واکنش به بحران بسیج کنند، که ارتباط و همکاری مهم بین کارکنان خط مقدم و فرماندهی حادثه را تسهیل کرد. بحران متکی به همکاری بین حرفه ای است، 3 تجزیه و تحلیل موفقیت ها و چالش های تعاملات بین حرفه ای در طول همه گیری بسیار مهم است. درک شرایط اجتماعی و ساختاری که کار چند تخصصی را در بیمارستانها تسهیل میکند یا مانع میشود و مطالعه تأثیر کووید-19 بر ماهیت کار چند تخصصی در آمادهسازی برای بحرانهای آینده مهم است. - اعضای تیم بهداشت و درمان خط مقدم پزشک در طول موج اولیه کووید-19.
2. روش ها
2.1. طراحی مطالعه
این مطالعه توصیفی کیفی، دیدگاههای HCWهای خط مقدم بستری را در مورد کار تیمی، ارتباطات و رهبری در یک مرکز پزشکی منطقهای VA در طول موج اولیه کووید-19 مورد بررسی قرار داد. شرکتکنندگان در مطالعه بخشی از تیمهایی بودند که دورههای بینرشتهای سازمانیافته روزانه (IDR) را قبل از همهگیری با هم انجام میدادند. این مطالعه بخشی از یک مطالعه بزرگتر بود که تجربیات HCWs و بیماران مبتلا به IDR در کنار بالین را بررسی کرد. این مطالعه توسط هیئت بررسی نهادی چندگانه کلرادو تأیید شد و رضایت آگاهانه اخذ شد (تأیید پروتکل COMIRB #19–2644)
2.2. تنظیمات و شرکت کنندگان
ما یک نمونه راحت از پرستاران کنار بالین، داروسازان، و هماهنگکنندههای مراقبت در واحدهای پزشکی بستری مراقبتهای حاد در مرکز پزشکی منطقهای کوه راکی VA (RMR VAMC)، یک بیمارستان منطقهای آکادمیک 88 تختی استخدام کردیم. همه هماهنگ كنندگان مراقبت از نظر آموزش پرستار بودند. شرکتکنندگان در صورتی واجد شرایط مطالعه بودند که به طور منظم در IDR کنار تخت قبل از همهگیری شرکت کرده بودند (بیش از 50 درصد شیفتهایشان). هدف ما نمونه برداری از کسانی بود که با IDR کنار تخت آشنا بودند و می توانستند در مورد تغییرات کار تیمی و ارتباطات در طول زمان نظر بدهند. IDR در بالین در ژوئن 2019 در بخشهای مراقبتهای حاد در RMR VAMC اجرا شد و شامل ورودی ساختاری از پزشکان، پرستاران، داروسازان و هماهنگکنندگان مراقبت درباره برنامههای مراقبت در کنار بالین بیمار بود. در طول موج شیوع کووید-19، تیمهای چند تخصصی به دور هم جمع شدن در خارج از اتاقهای بیماران ادامه دادند و سعی کردند با اعضای تیمی که از راه دور با فناوری صدا کار میکردند، تماس بگیرند.
2.3. جمع آوری داده ها
ما شرکت کنندگان را بین مارس و ژوئن 2020 از طریق ایمیل و شفاهی در گروه ها جذب کردیم. مشارکت داوطلبانه، محرمانه بود و به نقشها یا مسئولیتهای کاری مرتبط نبود. یک محقق کیفی با تجربه بدون رابطه قبلی با شرکتکنندگان، با شرکتکنندگان موافقت کرد و 18 مصاحبه نیمه ساختاریافته و عمیق از طریق تلفن (SRJ) انجام داد. نرخ مشارکت 46٪ (از 39 HCW واجد شرایط دعوت شده برای شرکت) بود. موضوعات مصاحبه شامل تجربیات کار تیمی و ارتباط در طول کووید-19، اثرات همه گیری بر IDR و رهبری، و مشارکت کارکنان در طول واکنش کووید-19 بود. مصاحبه ها تا 1 ساعت به طول انجامید و به صورت صوتی ضبط و به صورت حرفه ای رونویسی شد. ما مصاحبهها را انجام دادیم تا زمانی که به اشباع دادهها رسیدیم، جایی که هیچ اطلاعات جدیدی ظاهر نشد. 14،15 شرکتکننده برای قدردانی از وقت خود یک کارت هدیه 25 دلاری دریافت کردند.
2.4. تحلیل داده ها
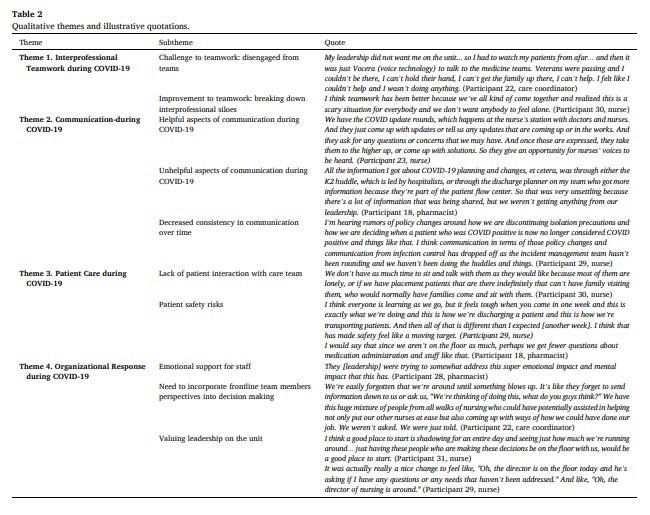
ما تجزیه و تحلیل را با استفاده از یک رویکرد تکراری، مبتنی بر تیم، استقرایی برای شناسایی مضامین کلیدی انجام دادیم. 16 با توجه به تحلیل موضوعی، تیم مطالعه یک کتاب کد تعریف و توافق کردند و دو کدگذار (SC, MP) همه رونوشت های شناسایی نشده را به طور مستقل کدگذاری کردند. ; هر گونه تفاوت در کدگذاری در طول فرآیند مقایسه و تطبیق داده شد. اول، ما رونوشت ها را به صورت قیاسی با استفاده از مجموعه ای موقت از کدهای استخراج شده از سوالات مصاحبه کدگذاری کردیم. کتاب کد شامل تعاریف هر کد برای چارچوب تجزیه و تحلیل است. سپس نتایج توسط تیم مطالعه (KM، SRJ، SC) برای تفسیر یافتههای اولیه بررسی و مورد بحث قرار گرفت. با استفاده از این بینش ها، چرخه دوم کدگذاری را به صورت استقرایی انجام دادیم تا الگوهای درون کدگذاری اولیه را جستجو کنیم و مضامین را شناسایی کنیم. 19 نقل قول های نماینده برای هر موضوع و زیرمضمون نشان داده شده در جدول 2 انتخاب شدند. نتایج با شرکتکنندگان برای بررسی آنها بهعنوان معیار اعتبار، و دو شرکتکننده با تأیید نتایج پاسخ دادند. 13 نرمافزار NVivo نسخه 12 برای مدیریت دادهها استفاده شد (QSR International Pty Ltd. (2020) NVivo).
ABSTRACT
Effective interprofessional teamwork serves an important role in successful crisis response. Responses to past public health crises have relied on interprofessional communication and trust to support healthcare worker (HCW) resiliency. To understand interprofessional interactions and perceptions of teamwork during the COVID19 response, we conducted in-depth semi-structured interviews with 18 inpatient HCWs (11 bedside nurses, 5 care coordinators, and 2 pharmacists) from one VA Medical Center between March and June 2020. Using thematic analysis, we identified four key themes that describe the strengths and challenges of interprofessional teamwork, communication, patient care, and organizational response during the initial COVID-19 surge. Interprofessional teams were fragmented. HCWs who transitioned to remote work lost their status on inpatient teams and struggled to provide pre-pandemic levels of quality of care. Conversely, interprofessional teamwork improved for HCWs who continued to work on inpatient units, where study participants described a decline in interprofessional hierarchies and an increase in mutual support. Participants described the need for timely, accurate, transparent communication as they faced new patient safety and communication challenges brought on by the pandemic. HCWs expressed a desire for sustained leadership support and inclusion in institutional decision-making. The challenges to teamwork, communication, and patient care reported in this study highlight the need for consistent, transparent communication and organizational response from hospital leadership during times of crisis.
1. Introduction
Throughout the COVID-19 pandemic, healthcare workers (HCW) in hospitals have faced significant professional and personal stressors resulting in disengagement with work and moral injury. They have battled inadequate supplies of personal protective equipment, anxiety about spreading the virus to loved ones, and concerns about rapidly changing inpatient protocols, procedures, and standards of practice.1,2 Interprofessional collaboration is a key factor in patient safety and successful communication, especially during the COVID-19 pandemic,3 as effective teamwork has been essential to supporting HCWs during responses to past crises.
Rates of stress, anxiety, and depression are high among frontline responders,5 and working during COVID-19 has resulted in chronic fatigue, insomnia, PTSD, and burnout among healthcare professionals.6 Effective communication and interprofessional teamwork are necessary when navigating crises and can have a significant role in staff empowerment and personal health. During the Severe Acute Respiratory Syndrome outbreak in 2003 and the Middle East Respiratory Syndrome outbreak in 2012, effective communication, collaboration, and trust across healthcare provider teams were crucial to crisis management. This created a sense of closeness and empowerment, which in turn fostered strong collective leadership and staff resilience.7,8 HCWs who worked during the H1N1 influenza pandemic in 2009 and the Ebola Virus Disease response in 2014 described the importance of receiving teamwork training and establishing clarity on team roles to support patient safety and personal health, and noted this as a key area for preparedness for future outbreaks.
During the current COVID-19 pandemic, several hospital systems succeeded in mobilizing frontline interprofessional teams to respond to the crisis, which facilitated crucial communication and collaboration between frontline staff and incident command.11,12 Because the organizational change necessary to tackle the COVID-19 crisis relies on interprofessional collaboration,3 it is critical to analyze successes with and challenges to interprofessional interactions during the pandemic. Understanding the social and structural conditions that facilitate or obstruct interprofessional work in hospital settings and studying the impact of COVID-19 on the nature of interprofessional work are important in preparing for future crises.4 In this study, we explored the perceptions of teamwork from non-physician frontline healthcare team members during the initial COVID-19 surge.
2. Methods
2.1. Study design
This qualitative descriptive study explored the perspectives of inpatient frontline HCWs on teamwork, communication, and leadership at a regional VA medical center during the initial COVID-19 surge. Study participants were a part of teams that performed daily structured bedside interdisciplinary rounds (IDR) together prior to the pandemic. This study was part of a larger study that investigated the experiences of HCWs and patients with bedside IDR. This study was approved by the Colorado Multiple Institutional Review Board and informed consent was obtained (protocol approval COMIRB #19–2644).
2.2. Setting and participants
We recruited a convenience sample of bedside nurses, pharmacists, and care coordinators on the acute care inpatient medical units at Rocky Mountain Regional VA Medical Center (RMR VAMC), an 88 bed academic regional hospital. All care coordinators were nurses by training. Participants were eligible for the study if they had participated regularly in bedside IDR prior to the pandemic (more than 50% of their shifts); our intent was to sample from those who were familiar with bedside IDR and could comment on changes to teamwork and communication over time. Bedside IDR was implemented on acute care wards at RMR VAMC in June 2019 and involved structured input from physicians, nurses, pharmacists, and care coordinators about care plans at the patient bedside. During the COVID-19 surge, interprofessional teams continued to round together outside of patient rooms, attempting to contact those team members who were working remotely by voice technology.
2.3. Data collection
We recruited participants between March and June of 2020 via email and word of mouth in team huddles. Participation was voluntary, confidential, and not tied to work roles or responsibilities.13 An experienced qualitative researcher without a pre-existing relationship to participants consented participants and conducted 18 semi-structured, in-depth interviews by phone (SRJ). The participation rate was 46% (of 39 eligible HCWs invited to participate). Interview topics included experiences with teamwork and communication during COVID-19, effects of the pandemic on IDR and leadership, and staff engagement during the COVID-19 response. Interviews lasted up to 1 hour and were audio-recorded and professionally transcribed. We conducted interviews until data saturation was reached, where no new information was emerging.14,15 Participants received a $25 gift card in appreciation of their time.
2.4. Data analysis
We conducted analysis using an iterative, team-based, inductive approach to identify key themes.16 Informed by thematic analysis,17,18 the study team defined and agreed upon a codebook and two coders (SC, MP) coded all de-identified transcripts independently; any differences in coding were compared and reconciled throughout the process. First, we coded transcripts deductively using a provisional set of codes drawn from the interview questions; the codebook included definitions of each code to frame the analysis. Results were then reviewed and discussed by the study team (KM, SRJ, SC) to interpret preliminary findings. Using these insights, we conducted a second cycle of coding inductively to look for patterns within the initial coding and identify themes.19 Representative quotes were selected for each theme and subtheme shown in Table 2. We performed member checking of findings, where we shared preliminary results with participants for their review as a measure of validity, and two participants responded confirming the results.13 NVivo software version 12 was used for data management (QSR International Pty Ltd. (2020) NVivo).
چکیده
1. مقدمه
2. روش ها
2.1. طراحی مطالعه
2.2. تنظیمات و شرکت کنندگان
2.3. جمع آوری داده ها
2.4. تحلیل داده ها
3. نتایج
3.1. موضوع 1. کار تیمی بین حرفه ای در طول کووید-19
3.2. موضوع 2. ارتباط در طول کووید-19
3.3. موضوع 3. مراقبت از بیمار در طول کووید-19
3.4. موضوع 4. پاسخ سازمانی در طول کووید-19
4. بحث
5. نتیجه گیری ها
منابع
ABSTRACT
1. Introduction
2. Methods
2.1. Study design
2.2. Setting and participants
2.3. Data collection
2.4. Data analysis
3. Results
3.1. Theme 1. Interprofessional teamwork during COVID-19
3.2. Theme 2. Communication during COVID-19
3.3. Theme 3. Patient care during COVID-19
3.4. Theme 4. Organizational response during COVID-19
4. Discussion
5. Conclusions
References